DoS Surgeons in the Media: “The Doctor is Out: Supporting Inclusion for LGBTQ+ Surgeons”
American College of Surgeons Bulletin
Tony Peregrin
March 8, 2023
“You come out as an LGBTQ+ individual virtually every day—it’s not like it happens once in a lifetime and you’re done,” said Harveshp D. Mogal, MD, MS, FACS, associate professor of surgery and section chief of complex abdominal oncology at the University of Washington (UW) Medical Center in Seattle.
![]() Dr. Mogal (he/him) is a member of the Association of Out Surgeons and Allies (AOSA), a relatively new organization comprising LGBTQ+ surgeons and allies from all surgical specialties.1
Dr. Mogal (he/him) is a member of the Association of Out Surgeons and Allies (AOSA), a relatively new organization comprising LGBTQ+ surgeons and allies from all surgical specialties.1
“For example, when you join a committee or you transition into a leadership position, you still face a lot of unknowns in terms of how people are going to respond to you as an out surgeon,” he added. “My hope is that with more of us joining organizations like AOSA, we will learn to normalize this process, and that eventually, being LGBTQ+ will just be part of the fabric of surgery rather than something that we have to struggle against because it’s not as accepted as it should be.”
The idea to form a group of LGBTQ+ surgeons and allies emerged on MedTwitter toward the end of 2018. AOSA—which had its inaugural founders’ meeting at Clinical Congress 2019 in San Francisco, CA—is committed to creating “a space for LGBTQ+ surgeons and trainees that promotes a dignified and successful surgical career without stigma, judgment, or discrimination,” according to the group’s mission statement. “We aim to achieve this through a combination of outreach, education, mentorship, and professional development.”1,2
 “If you’re not out, you constantly have to make sure not to make a comment about your personal life, about your partner, and so on. And that’s a lot of emotional energy when you’re trying to focus on operating.” —Dr. Nicole Goulet
“If you’re not out, you constantly have to make sure not to make a comment about your personal life, about your partner, and so on. And that’s a lot of emotional energy when you’re trying to focus on operating.” —Dr. Nicole Goulet
AOSA held its first business meeting at Clinical Congress 2022 in San Diego, CA, during which members elected individuals to fill officer and chair positions within the organization.
“The decision to go into surgery when you identify as queer is a big one,” said Nicole Goulet, MD, FACS, (she/her), president of AOSA and director of the surgical intensive care unit at New York University Langone Hospital in Brooklyn. “While it’s getting better, there are still comments that are made by surgeons in the operating room that include derogatory terminology about being gay, and if you’re a surgeon who is not out, you think ‘Geez, I certainly need to make sure I hide this.’”
An article, written by members of the Resident and Associate Society of the ACS and published in the January 2021 issue of the ACS Bulletin, noted that “…it is unsurprising that LGBTQ+ surgery residents fear disclosure and instead pretend to be heterosexual to avoid potential problems. This approach not only is unhealthy, but also decreases the opportunity for those surgeons with ingenuous views to have meaningful interactions with LGBTQ+ people, which could help challenge biases.”3
Dr. Goulet cited data from two recent studies that provide additional context to the experiences of some LGBTQ+ surgical trainees.
A 2014 survey of 388 general surgery residents found that for those who identified as LGBTQ+, 57% reported actively concealing their sexual orientation from fellow residents owing to fear of rejection, and 52% from surgical attending physicians owing to fear of poor evaluations.4,5 Among the surgical residents who experienced homophobic remarks, none reported the incident to leadership due to fear of reprisal among other reasons, according to Dr. Goulet.
A larger study published in 2019 surveyed 6,562 general surgery residents and found that for those who identified as LGBTQ+, 46.8% reported sexual harassment, 58.9% discrimination, and 75.2% bullying.4,6 The study authors noted that while LGBTQ+ respondents were just as likely to be satisfied with their decision to become a surgeon, they were twice as likely to consider leaving their program and/or had suicidal thoughts in the past year.
“We’d all like to say that you can leave your personal life at home, but that’s just not the case,” said Dr. Goulet. “In surgery, we spend so much time together in residency, and then as colleagues in the operating room—and if you’re not out, you constantly have to make sure not to make a comment about your personal life, about your partner, and so on. And that’s a lot of emotional energy when you’re trying to focus on operating.”
“We are kind of exhausted being the outsiders or the ‘others’ within the group, where we are kind of expected to bring our full professional identity to work, but keep our personal identity completely divested from it,” added Dr. Mogal. “That being said, I think, in general, people in the workforce today are more open about expressing their full identity without fear of retribution or discrimination. But particularly in surgery, that change has come very slowly. And arguably, it still isn’t fully there, which is why we have organizations like the AOSA.”
In order to propel this positive change even further, it is important to examine LGBTQ+ equity through an intersectional lens, which considers the racial and ethnic backgrounds, differing abilities, and other variables and identities that comprise the LGBTQ+ community.7
Advancing intersectional equity starts by recognizing that certain individuals face overlapping forms of discrimination, such as an openly gay surgeon who also identifies as Black or has a disability. In order to support meaningful inclusivity for all LGBTQ+ surgeons and other healthcare providers, it is essential to cultivate an intersectional approach to policy development, recruitment, and training that takes into consideration the complex challenges of all marginalized individuals.
Primary Aims of the AOSA
The AOSA, which currently has 200 members, has four main objectives:
- Reduce explicit and implicit bias
- Enhance systemic support
- Foster mentorship
- Support leadership opportunities and promotion
“In the short term, we want to grow our membership and raise awareness and visibility about who we are,” explained Dr. Goulet. “And secondarily, a key component of our short-term goal is to provide advice, guidance, and education to other surgical organizations and societies.”
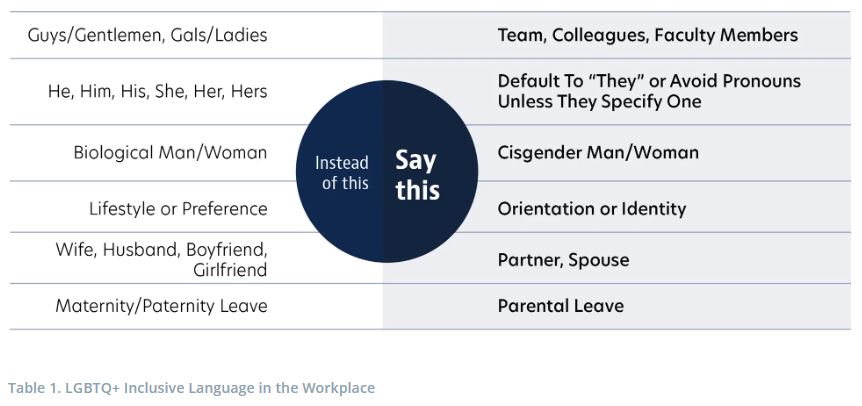
One example of educational outreach that could immediately enhance the narrative around LGBTQ+ individuals in the healthcare setting: The use of correct terminology, including pronouns.
In general, asking others their pronouns and names is a good place to start, according to Drs. Goulet and Mogal. It is recommended that surgeons and other healthcare providers avoid assuming individuals are cisgender and heterosexual and find teachable moments to advise colleagues in using appropriate and inclusive language if such a situation occurs8 (see Table 1).
“Asking what people’s pronouns are, or introducing yourself with that information, helps to normalize this process,” said Dr. Goulet. “As we start building that culture of having this be the norm, it creates an open conversation for everyone you work with and for our patients as well. Patients are going to hear these conversations and will, hopefully, be more likely to share things with you as their provider that they wouldn’t have shared otherwise.”
As for AOSA’s long-term goals, developing a robust mentorship network is a benefit that will continue to evolve as membership numbers tick upward.
“Our members are really looking for a mentor they can reach out to if they are having trouble with their program or if they have questions about how to apply for a job if they are out,” Dr. Goulet said. “We have a lot of people in the AOSA who are very comfortable with where they’re at with being out, and they can provide advice to help others along their surgical career path.”
 “It is meaningful for LGBTQ+ trainees to be mentored by LGBTQ+ faculty because it’s important to see yourself mirrored in someone who is successful and continuing to succeed.” —Dr. Harveshp Mogal
“It is meaningful for LGBTQ+ trainees to be mentored by LGBTQ+ faculty because it’s important to see yourself mirrored in someone who is successful and continuing to succeed.” —Dr. Harveshp Mogal
Supporting LGBTQ+ Trainees
It is important to “create safe and welcoming environments for our trainees so that they can not only survive the rigors of training, but have the same opportunities to thrive as their gender-conforming and heterosexual counterparts,” noted Dr. Mogal during a recent webinar.8
Dr. Mogal outlined four levels where LGBTQ+ individuals and allies can actively promote diversity in the surgical workforce (see Table 2).8
- Individual: Participate as an affirming and active bystander, which could include normalizing personal life discussions at work, correcting false assumptions or stereotypes, apologizing and promising to do better, when necessary
- Departmental: Engage in proactive and intentional recruitment, support targeted mentorship and sponsorship opportunities, and include LGBTQ+ individuals within the formal settings of committees and councils
- Institutional: Develop inclusive categories on admissions forms and surveys and be mindful of including the different types of gender identities that people identify with; expand benefits to spouses and same-sex domestic partners, support zero tolerance for bullying and harassment, along with a confidential reporting process
- National: Standardize LGBTQ+ curriculum within medical and surgical training, develop statements from leadership validating the experiences of LGBTQ+ individuals, and promote collaboration between national surgical organizations and groups like the AOSA
 Dr. Mogal emphasized the need for increased visibility and allyship at all levels, particularly regarding the toll of the minority tax, which occurs when recruiting, mentoring, and educating others is disproportionately assigned to underrepresented minorities, due to the assumption that these individuals are uniquely qualified to fulfill these roles.9
Dr. Mogal emphasized the need for increased visibility and allyship at all levels, particularly regarding the toll of the minority tax, which occurs when recruiting, mentoring, and educating others is disproportionately assigned to underrepresented minorities, due to the assumption that these individuals are uniquely qualified to fulfill these roles.9
“The burden of mentoring junior faculty, residents, or trainees tends to fall on those who identify similarly,” said Dr. Mogal. “It is meaningful for LGBTQ+ trainees to be mentored by LGBTQ+ faculty because it’s important to see yourself mirrored in someone who is successful and continuing to succeed. But it’s equally important that those residents have a diverse perspective in terms of non-LGBTQ+ faculty because their academic interests may not necessarily align with somebody who’s LGBTQ+.”
Dr. Mogal said it is equally important to ensure that other leaders mentor these individuals.
“It’s very easy to delegate diversity issues to the underrepresented,” said Douglas E. Wood, MD, FACS, FRCSEd, an ACS Regent and the Henry N. Harkins Professor and chair of the Department of Surgery at UW. “While these individuals have a lived experience and content expertise, it is an added burden, a minority tax, to expect them to exclusively lead change. I think surgeons, like myself, have a responsibility to own the inclusiveness, and to actually lead it with guidance from our LGBTQ+ colleagues and friends, who can help us get it right.”
 “They change me. They help this cisgender, straight man to have a better sense of empathy, and they help minimize the stigma that we might have for the patients who we care for.” —Dr. Douglas Wood
“They change me. They help this cisgender, straight man to have a better sense of empathy, and they help minimize the stigma that we might have for the patients who we care for.” —Dr. Douglas Wood
The Role of the Straight Ally
Straight, cisgender faculty members can provide support for LGBTQ+ individuals by first acknowledging that this disparity exists and then by playing an active role in developing safe spaces for residents and trainees.
“My privilege has given me the opportunity to be a department chair and it has given me the privilege of being a Regent,” Dr. Wood said. “These are positions of influence where I can actually do something. That’s why it should fall on me to lean in and be involved. And that is why I am a proud individual and institutional member of the AOSA.”
Dr. Goulet estimates that about 10% of AOSA membership is composed of individuals who do not identify as LGBTQ+ based on information gleaned from the organization’s membership application. She said the overall reaction to the AOSA and its mission has been “surprisingly positive.”
“A lot of other surgical organizations and people outside of our group have been really supportive because they realize that our mission is important.”
Dr. Goulet has some simple, but powerful advice for all surgeon allies to help foster an inclusive environment: if you make a mistake, own it, apologize, and learn from the experience.
“Earlier in my career, I went for a job interview after fellowship and one of the older male surgeons who was interviewing me failed to look at my CV carefully and didn’t see all the LGBTQ+ stuff on there,” said Dr. Goulet. “He asked all the illegal questions you’re not supposed to ask during an interview, questions about kids and a husband. At that point in my career, I had already decided that I was going to be myself in these interviews, so I corrected him, he got flustered, and he wasn’t sure what to say.”
Her advice in these situations is to simply say “I’m so sorry” to change the cadence of the conversation, and to think carefully before getting into a similar position. “I always say nobody’s perfect. We’re all learning and sometimes we misspeak,” said Dr. Goulet.
“Surgery has been a very macho, very hetero and homophobic specialty,” said Dr. Wood. “I have heard so many casual dialogues that have been disrespectful to LGBTQ+ individuals of all types, whether it’s a trans person in the emergency room or a gay man who is undergoing a surgical procedure.”
According to Dr. Wood, one of the most impactful ways to influence the culture in surgery is to be more actively inclusive of LGBTQ+ surgeons.
“They change me. They help this cisgender, straight man to have a better sense of empathy, and they help minimize the stigma that we might have for the patients who we care for,” he said. “Organizations like the ASOA are shining a bright light on the issues experienced by many LGBTQ+ surgeons, and they are intentional in their efforts to make our residency programs and healthcare systems more welcoming and inclusive.”
Tony Peregrin is Managing Editor, Special Projects, in the ACS Division of Integrated Communications in Chicago, IL.
References
- Association of Out Surgeons and Allies. Mission statement. Available at: https://www.outsurgeons.org. Accessed February 7, 2023.
- St. John A, Goulet N. Enhancing diversity in surgery: Association of Out Surgeons and Allies, a new society to support and promote lesbian, gay, bisexual, transgender and queer surgeon. Am Surg. 2022;88(12):2810-2816.
- Tracy BM, Koo K, Strong B, Poulson M, et al. Glass ceilings and sticky floors: Examining diversity and inclusion in the surgical workforce. Bull Am Coll Surg. 2021;106(1):31-36.
- Cortina CS, Williamson AJ, Goulet ND. Progress, barriers, and the future of LGBTQ+ surgeons in academic surgery. Am J Surg. 2022 Jul;224(1 Pt B):294-295.
- Lee KP, Kelz RR, Dub´e B, Morris JB. Attitude and perceptions of the other underrepresented minority in surgery. J Surg Educ. 2014;71(6):e47–e52.
- Heiderscheit EA, Schlick CJR, Ellis RJ, et al. Experiences of LGBTQ+ residents in US general surgery training programs. JAMA Surg. 2022;157(1):23–32.
- Olsen. B. How intersectionality affects the LGBTQ+ community. LGBTQ and ALL. Available at: https://www.lgbtqandall.com/how-intersectionality-affects-the-lgbtq-community. Accessed February 21, 2023.
- AIS Channel. Inclusivity in Surgery: An LGBTQIA+ Perspective. November 22, 2022. Available at: https://aischannel.com/live-surgery/inclusivity-in-surgery-an-lgbtqia-perspective. (Log-in/registration required). February 7, 2023.
- Nitkin K. The majority subsidy. Hopkins Medicine Magazine. Winter 2020. Available at: https://www.hopkinsmedicine.org/news/articles/the-majority-subsidy. Accessed February 7, 2023.